What are the key issues / trends regarding ethics, autonomy and academic freedom in your context? What impact does this have on staff?
Key observations / take always from this evening’s class and readings:
- PROCESS – the process required for ethics approval for research in HE can hamper research. For example: cross institutional collaboration where there are differing standards and timings of meetings reduces efficiency and delays the process. I have seen this at play in research projects undertaken by a colleague Rehabilitation Physician who is doing her PhD in rehabilitation models of care in road trauma across multiple sites – the research was delayed substantially because of the timing of ethics meetings and minor edits and modifications required by individual hospitals / institutions. Identification of this as a potential delay in a project should occur and be strategically planned for in the planning phase of a research project.
- NEED FOR APPROVAL – EVERYTHING IS EQUAL BUT SOME THINGS ARE MORE EQUAL THAN OTHERS – there was a fascinating discussion about the differences and similarities between research and evaluation (refer back to my post from week 5). One body of work, for example, reviewing the effectiveness of a particular teaching method could be used for two different purposes: for evaluation or for research…and the factor which determines whether or not ethics approval is required hinges on what the research is labelled as: whether it is labelled as “research” (and therefore may be published) or “evaluation” (or quality assurance). An argument could be made that “what is good for the goose is good for the gander” and that UNSW’s research policy “All UNSW staff or students who intend to conduct research as part of a degree must apply for approval from the appropriate ethics review body” should be applied to the letter of the law. However, if this were applied to the letter of the law, evaluation and therefore progress in education could be hampered……but is it a fine line!
- THE ROLES OF THE ACADEMIC WHEN THINGS ARE GOING WELL: We discussed the three key roles of the academic as being: teaching, research and service (as a hospital based conjoint lecturer, I have a fourth leg on my stool being a clinician)…….the service role can be both internal and external…..the external role can include being sought to provide public comment on a particular topic……..because they may be seen as being “ethical” with the public perception of an academic as being independent, knowledgeable and impartial. In the situation where the academic’s opinions and behaviour are in alignment with the institution, there are no issues.
- ROTTON APPLES: When an academic engages in “unethical”” behaviour, this can have negative implications on a number of levels – on the reputation of the individual of course, but also on other academics at that institution and the institution itself, raising questions about other work done at that institution. As they say “mud sticks” and many can be “tarred with the same brush” as a consequence of unethical behaviour or a minority of individuals. This is a scenario with which I have been all too familiar in the last months following a “scandal” involving clinicians in another department at a hospital I work at , I have found myself answering questions about the integrity of other clinicians at the hospital. More subtle than this, however, are situations wehere an academic is oeprating on the fringes of what is “acceptable” in a particular institution. Clear delineation of expectations are necessary, balanced against the individual’s right to academic freedom.
- ACADEMIC FREEDOM VERSUS PROCEDURAL / SUBSTANTIVE AUTONOMY. More subtle than overt “rotten apples” are situations where an academic is opirating on the fringes of what is “acceptable” in a particular institution. Clear delineation of expectations are necessary, balanced against the individual’s right to academic freedom. Ethicak questions arise when the independence of the individual is at odds with the direction or opinion of the institution. How this is resolved and which perspective takes precedence depends on the culture of the institution, the issues at stake and the implications……
- FREEDOM VERSUS AUTONOMY: A PERSONAL TALE: I have been in a position where a program I set up with institutional support won a national industry award and was a finalist in a state government awards process……both of which were decided after the institution, because of funding pressures decided to cut the funding for that program. I was directed that in my public comments after these award ceremonies, I was not to mention the cutting of the funding……..procedural autonomy definitely trumped academic freedom in that case and I am still left with a very bitter taste in my mouth and cynicism in my heart.
- FUNDING CONFLICTS – beyond the more overt ethical implications of “rotten apples” in HE, there are other ethical implications for funding in HE. For example, subtle influences from the incumbent government on research or teaching priorities for particular institutions, or perhaps the indirect influence of societal groups to whom a particular political party is seeking a favourable impression. Or where public funding is less available, funding shifts to private sources including individual donors and corporate entities which have the potential for as much influence on the operation and content of universities’ outputs as political influence. In these scenarios, there is a real potential for conflict between the institution’s autonomy and the influence of these other individuals / entities, particularly where their motives or priorities are at odds. Not only do institution’s need to do the right thing, they also need to be seen to be doing the right thing too, the concept as mentioned by my fellow scholar as “independence of mind and independence of appearance”.
Research and teaching nexus
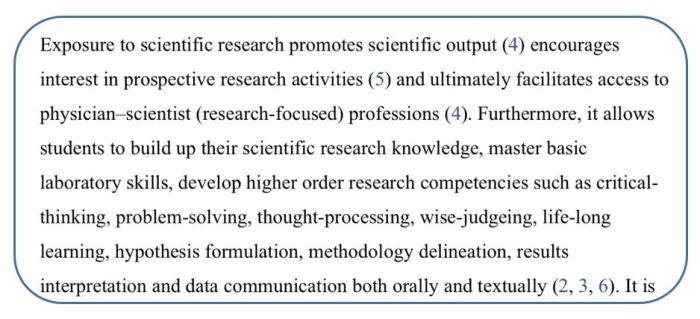
Incorporating research into education programs in HE offers advantages from many perspectives, including teachers, students, the faculty, the insitution and for society at large. Specific to medical education, the key advantages were well summarised by Abu-Zaid and Alkattan (2013)
I found the categorisation of research in HE put by Healey, Jenkins and Lea (2014) a useful framework with which to consider the role of research in the HE setting in which I am primarily involved (post-graduate specialist teaching). Equally, the application of Boyer’s scholarships to research activities was a very useful way of conceptualising research activities, and I was struck by the parallels between Boyer’s scholarships and Healey, Jenkins and Lea’s (2014) research classification. These parallels and insights are explored in the table below.

Conclusion
A consideration of the role of ethics in higher education and research is vital. Standards and expectations need to be both clearly articulated, and communicated in a manner which is understandable and practical and these standards and expectations need to be applied in a judicious and equitable manner. Opportunities to review ethical processes and standards must be available and staff and students at all levels need to have authentic input into these processes. Changes in HE, particularly as it pertains to changes in societal standards and the introduction of new technologies demands that processes regarding ethics be reviewed and possibly re-conceptualised at a more frequent rate.
In summary, the ratio and importance of the scholarship of research in education varies greatly, with that variation informed and influenced by a number of key factors, including the priorities, culture and history of individual teachers, work groups, schools, faculties and the institution as a whole. Frank discussions about the relative focus and importance of research in education is essential, with the allowance of flexibility to account for the heterogeneity of elements which make up the institution.
References
- Abu-Zaid, A., & Alkattan, K. (2013). Integration of scientific research training into undergraduate medical education: a reminder call. Medical education online, 18.
- Boyer, E. L. (1990). Scholarship reconsidered: Priorities of the professoriate. Princeton University Press, 3175 Princeton Pike, Lawrenceville, NJ 08648..
- Burgoyne, L., O’Flynn, S., & Boylan, G. (2010). Undergraduate medical research: the student perspective. Medical education online, 15(1), 5212.
- Healey, M., Jenkins, A., & Lea, J. (2014). Developing research-based curricula in college-based higher education. York: HEA.
- RACP. (2013). Rehabilitation Medicine: Advanced Training Curriuclum. Retrieved 2017_06_05 from: https://www.racp.edu.au/docs/default-source/default-document-library/at-afrm-rehabilitation-medicine-curriculum.pdf.
- RACP. (2016). Rehabilitation Medicine: Program Requirements Handbook. Retrieved 2017_06_05 from: https://www.racp.edu.au/docs/default-source/default-document-library/at-rehabilitation-medicine-hb-2016.pdf?sfvrsn=2
- UNSW. (2016). Applying for Ethics Approval”. Retrieved 2017_05_23 from: https://research.unsw.edu.au/applying-ethics-approval

 trusty
trusty